This is a 75 year-old female with a history of rheumatoid arthritis presents to office with several years of progressive neck pain.
She also reports 3 months of numbness in her hands; denies weakness but reports apraxia. She also report ataxia – feels off balance.
Her neurological examination reveals loss of sensation in her hands and hyperreflexia.

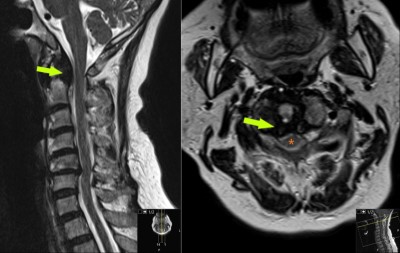
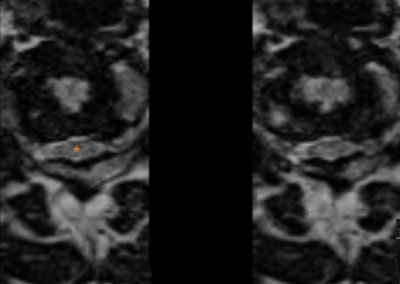
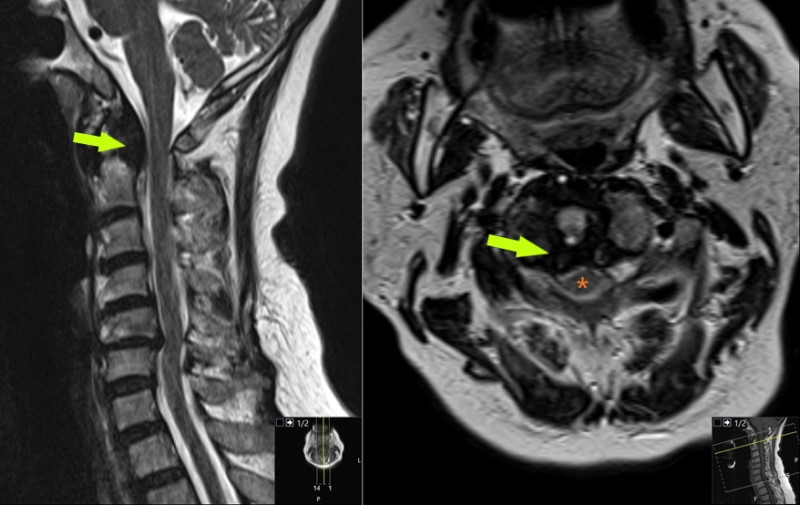
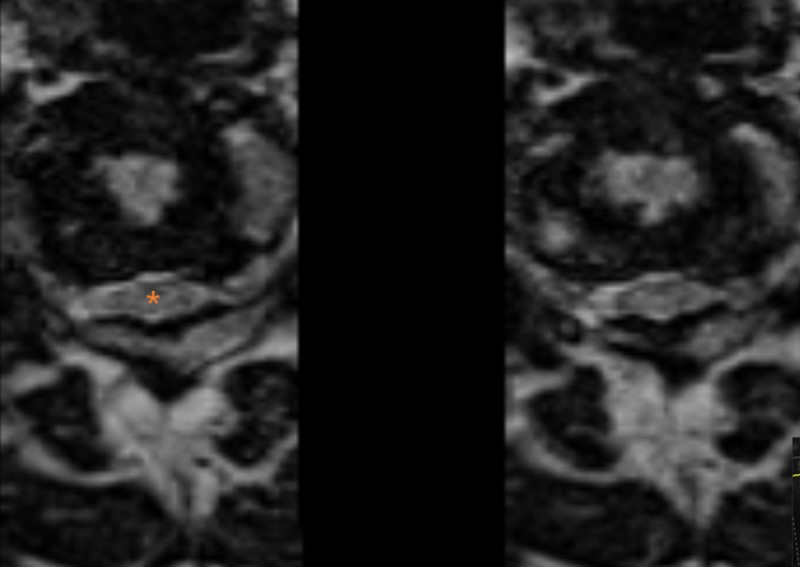
: Sagittal MRI images obtained just prior to surgery. They show a stable soft tissue mass behind the odontoid process of C2 (compare with Figure 1). It is compressing the spinal cord (yellow arrow on left). There is also evidence of instability at C1-2. Additionally, there is disc displacement at C5/6 causing some canal stenosis (yellow arrow on right).
- All
- Pre-Op
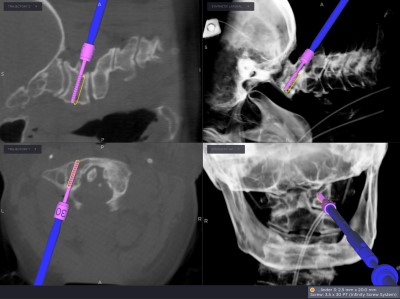
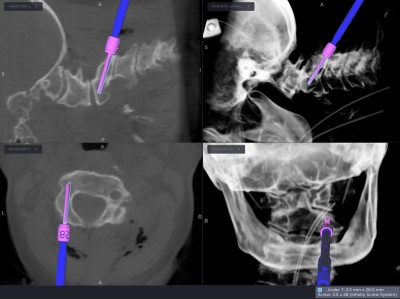
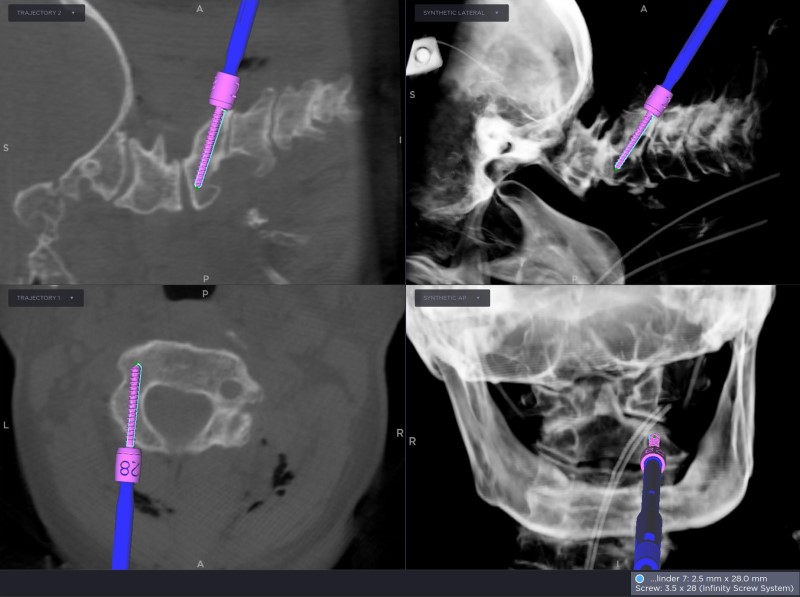
- Intra-op
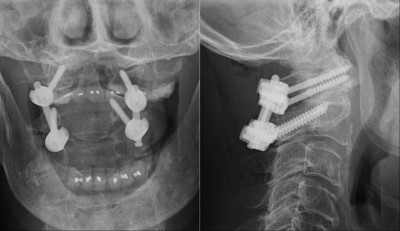
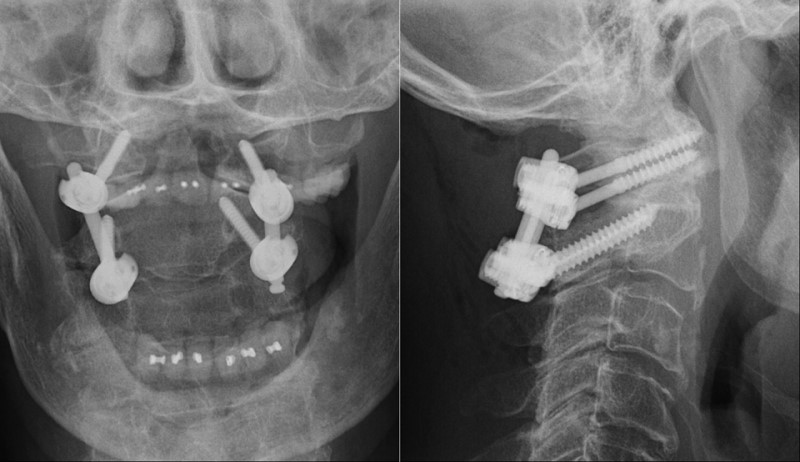
- Post-op
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}