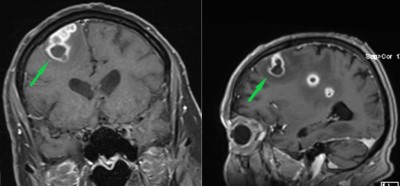
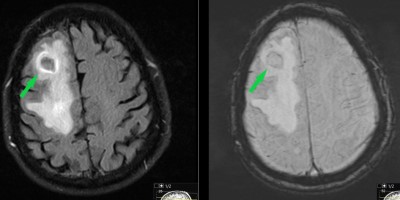
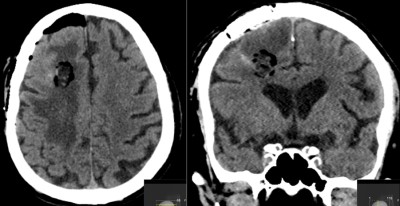
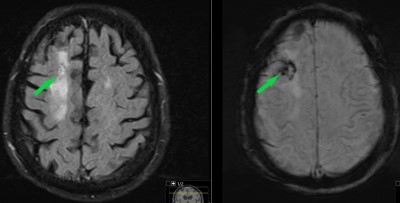
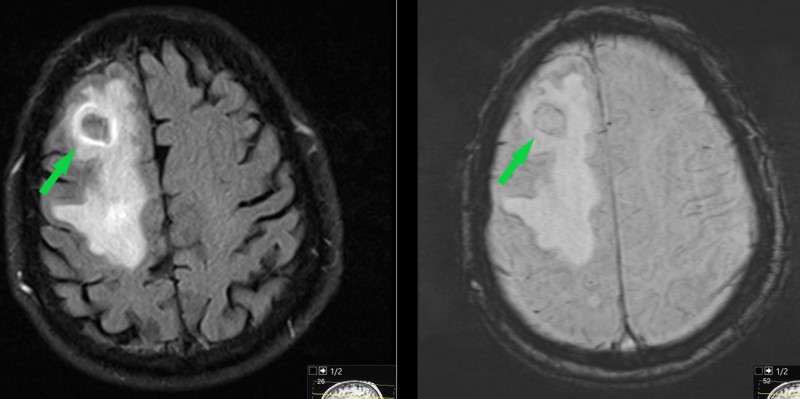
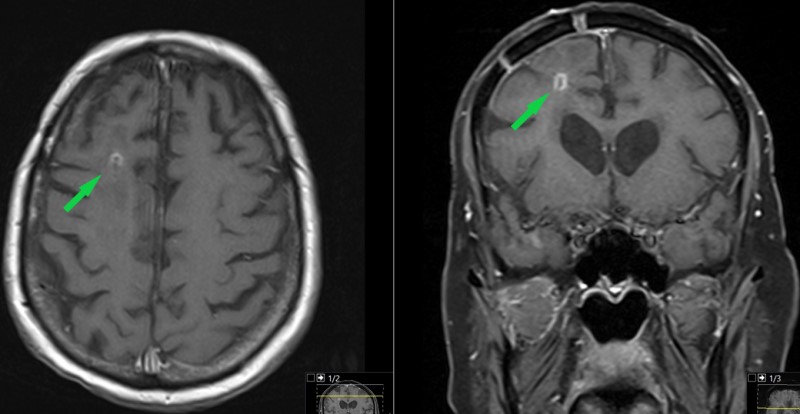
This is a 90 year old male who presented to the ER with several days of progressive left-sided weakness in arm more than leg which led to fall at home prompting presentation to ER. The past medical history is relatively unremarkable other than pancytopenia (low blood cell counts).
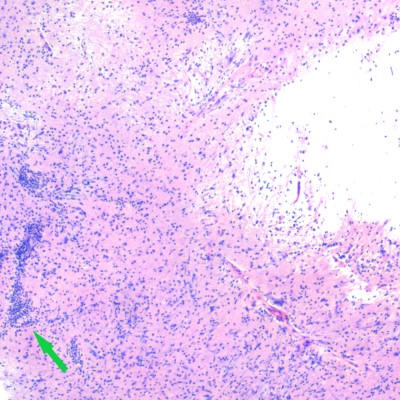
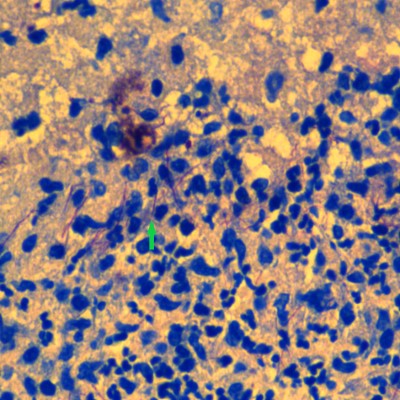
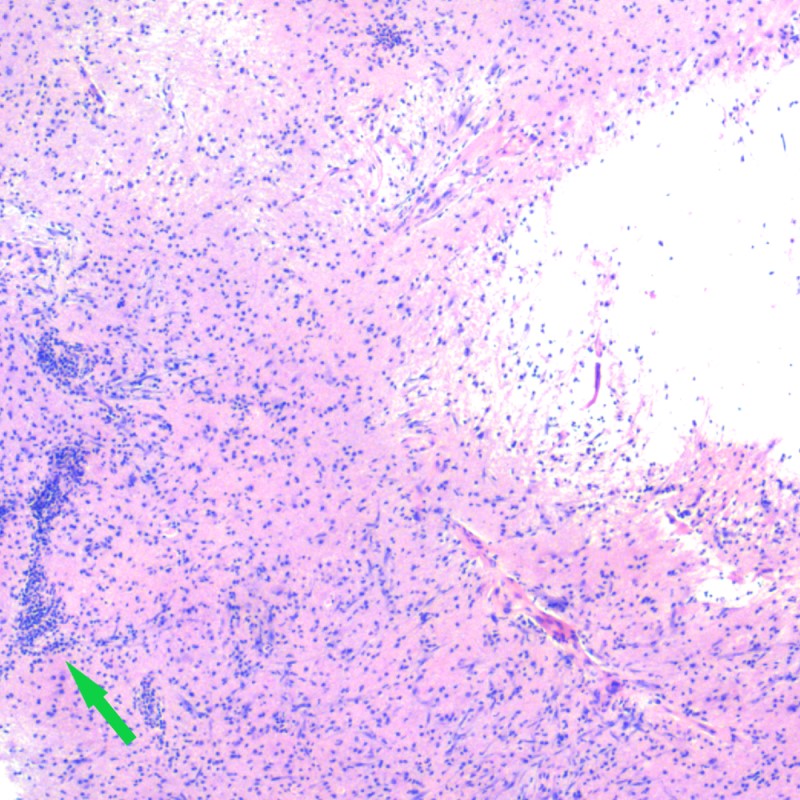
Photo micrograph of patient's pathologic specimen. This H&E stain shows brain tissue (pink) with an inflammatory infiltrate (multiple purple dots throughout the image). There is a cluster of these inflammatory cells above the tip of the green arrow. While abnormal, this does not provide the diagnosis.
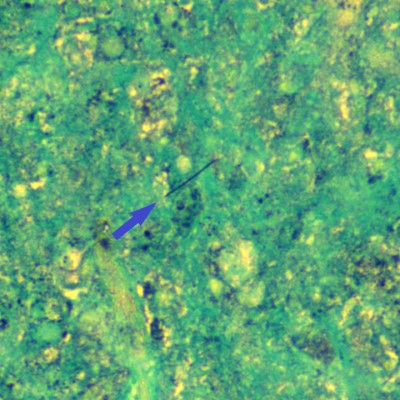
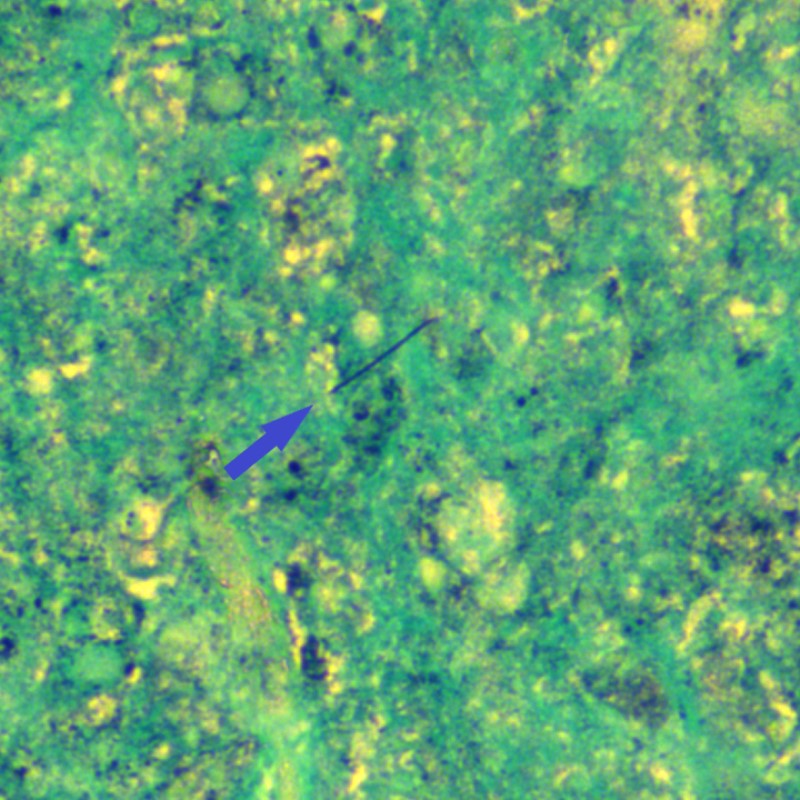
Photo micrograph of GMS (Grocott’s Methenamine Silver) stain of pathologic specimen. It also demonstrates a filamentous microbe consistent with infection (blue arrow).
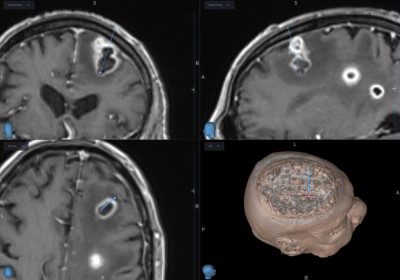
Microbiological specimens collected during craniotomy grow Nocardia araoensis. It is susceptible to multiple antibiotics. Patient is treated with antibiotics.
- All
- Pre-Op
- Intra-op
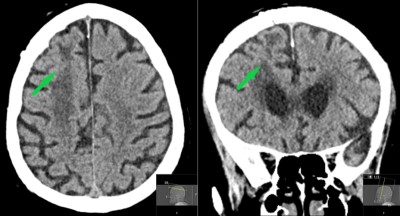
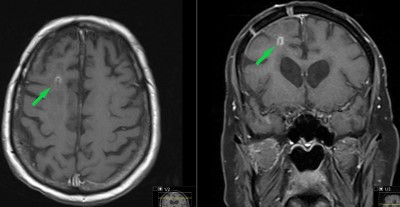
- Post-op
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}